Health
“It’s no longer an opioid epidemic,” said Dr. Cara Poland, an associate professor at the Michigan State University College of Human Medicine. “This is an addiction crisis.”
Dr. Nic Helmstetter crab-walked down a steep, rain-slicked trail into a grove of maple and cottonwood trees to his destination: a dozen tents in a clearing by the Kalamazoo River, surrounded by the detritus of lives perpetually on the move. Discarded red plastic cups. A wet sock flung over a bush. A carpet square. And scattered across the forest floor: orange vial caps and used syringes.
Kalamazoo, a small city in Western Michigan, is a way station along the drug trafficking corridor between Chicago and Detroit. In its parks, under railroad overpasses and here in the woods, people ensnared by drugs scramble to survive. Helmstetter, who makes weekly primary care rounds with a program called Street Medicine Kalamazoo, carried medications to reverse overdoses, blunt cravings and ease withdrawal-induced nausea.
But increasingly, the utility of these therapies, developed to address the decades-old opioid crisis, is diminishing. They work to counteract the most devastating effects of fentanyl and heroin, but most users now routinely test positive for other substances too, predominantly stimulants such as cocaine and methamphetamine, for which there are no approved medications.
Rachel, 35, her hair dyed a silvery lavender, ran to greet Helmstetter. She takes the medicine buprenorphine, which acts to dull her body’s yearning for opioids, but she was not ready to let go of meth.
“I prefer both, actually,” she said. “I like to be up and down at the same time.”
The United States is in a new and perilous period in its battle against illicit drugs. The scourge is not only opioids, such as fentanyl, but a rapidly growing practice that the Centers for Disease Control and Prevention labels “polysubstance use.”
Over the last three years, studies of people addicted to opioids (a population estimated to be in the millions) have consistently shown that between 70% and 80% also take other illicit substances, a shift that is stymieing treatment efforts and confounding state, local and federal policies.
“It’s no longer an opioid epidemic,” said Dr. Cara Poland, an associate professor at the Michigan State University College of Human Medicine. “This is an addiction crisis.”


The non-opioid drugs include those relatively new to the street, such as the animal tranquilizer xylazine, which can char human flesh, anti-anxiety medications including Valium and Klonopin and older recreational stimulants such as cocaine and meth. Dealers sell these drugs, plus counterfeit Percocet and Xanax pills, often mixed with fentanyl.
The incursion of meth has been particularly problematic. Not only is there is no approved medical treatment for meth addiction, but meth can also undercut the effectiveness of opioid addiction therapies. Meth explodes the pleasure receptors, but also induces paranoia and hallucinations, works like a slow acid on teeth and heart valves and can inflict long-lasting brain changes.
The Biden administration has been pouring billions into opioid interventions and policing traffickers, but has otherwise lagged in keeping pace with the evolution of drug use. There has been comparatively little discussion about meth and cocaine, despite the fact that during the 12-month period ending in May 2023, more than 34,000 deaths were attributed to methamphetamine and 28,000 to cocaine, according to provisional federal data.
Just last month, the Food and Drug Administration issued draft guidelines for the development of therapies for stimulant-use disorders “critically needed to address treatment gaps.”
In the Street Medicine van up the road from the tents, Dr. Sravani Alluri, the program’s director and a family medicine physician, gave Rachel an injection of antipsychotic medicine and then sorted through lab results showing the chilling omnipresence of numerous substances.
Patient No. 1: positive for fentanyl, methamphetamine and xylazine.
Patient No. 2: positive for amphetamine, methamphetamine, cocaine, THC and gabapentin, a prescription painkiller whose misuse is on the rise.
Patient No. 3: positive for fentanyl, methamphetamine, THC and xylazine.
The spread of super meth

“Treating someone for opiates is relatively easy,” said Dr. Paul Trowbridge, the addiction medicine specialist at the Trinity Health Recovery Medicine clinic in Grand Rapids, Michigan, an hour north of Kalamazoo. That’s largely because of buprenorphine and methadone, federally approved medications with years of evidence attesting to their effectiveness in subduing opioid cravings, and Narcan, an over-the-counter nasal spray that reverses opioid overdoses.
But meth, he said, “is a monster.”
His patients typically have either Medicaid or private health insurance and a roof over their heads, even if it’s a shelter. Many have steady jobs — dental hygienists, construction workers, tech sales people.
Still, the challenges of helping them are daunting.
Their use of multiple drugs is not always voluntary. Dealers can be sloppy, Trowbridge said, or intentionally salt one drug with another, to bind customers to the new mix.
“It’s really unpredictable what people are buying, which makes it so dangerous for them,” he said. “It’s a killing field out there.”
Some opioid users seek the fireworks of meth and other stimulants to offset the warm, sleepy embrace of opioids. Some use meth to stay awake to ward off thieves and rapists.

Medications such as methadone can safely replace more destructive opioids and satiate the brain’s opioid receptors. But subduing the urge for stimulants, which set off the release of stratospheric levels of the brain chemicals dopamine and serotonin, is more complex, involving many unknowns. And Narcan, which has saved at least hundreds of thousands who overdosed on opioids, has no effect on stimulants.
Moreover, depending on whether the user routinely turns to cocaine, meth or prescription amphetamine, side effects, responses and behavior patterns vary greatly.
“The truth is, we really don’t have a good answer at this point as to why it’s so challenging to develop these treatments,” said Marta Sokolowska, the deputy director for substance use and behavioral health at the FDA’s Center for Drug Evaluation and Research.
Last year, according to preliminary federal data, stimulants were present in 42% of overdose deaths that involved opioids.
Like opioids, which originally came from the poppy, meth started out as a plant-based product, derived from the herb ephedra. Now, both drugs can be produced in bulk synthetically and cheaply. They each pack a potentially lethal, addictive wallop far stronger than their precursors.
In recent decades, opioids grew so dominant that meth and its stimulant cousins proliferated in the shadows.
A decade or so ago, Mexican drug lords figured out how to mass-produce a synthetic “super meth.” It has provoked what some researchers are calling a second meth epidemic.
Popular up and down the West Coast, super meth from Mexican and American labs has been marching east and south and into parts of the Midwest, including Grand Rapids and Kalamazoo.


Users inject, snort or ingest meth, often seeking to prolong its euphoria with binges that can last for days. Meth can also trigger violence and psychosis that emergency doctors can mistake for schizophrenia. Its long-term effects include anhedonia and memory loss.
To help patients cut back on meth, some doctors prescribe Adderall, a drug for attention deficit hyperactivity disorder that is also a stimulant. But that avenue is narrowing, because of the drug’s nationwide shortage.
People addicted to multiple substances are far more resistant to going into treatment than single-substance users, addiction medicine experts say.
Trowbridge said some opioid patients can become stable enough to progress to monthly injectable buprenorphine. But if they are also using meth, that treatment plan often collapses.
The paranoia and hallucinations caused by meth disorient them, he said. One patient threw himself in a river to escape nonexistent people who were chasing him. Others insisted that dumpsters were talking to them or that color-coded cars were sending them messages.
So they skip appointments, returning only “when they start to hit withdrawal and realize their opioid injection is wearing off,” he said.
At the clinic that day, at least four patients were no-shows.
“We’re just trying to not have them have a heroin habit,” Trowbridge said. “But then they’re off on a meth run.”
Meth, opioids and pregnancy

Sami, 30, who is addicted to meth and heroin, is pregnant with her third child, due in December.
This is her second pregnancy with the Great Moms clinic, a Grand Rapids program through Corewell Health that supports pregnant women who struggle with drug use. Citing privacy concerns in not sharing her full name, Sami, who has long, dark hair and a life-hardened jawline, had been fastidious about keeping her appointments. She is trying to get it right this time.
Three years ago, the clinic prescribed buprenorphine to help Sami contain heroin urges during her second pregnancy.
But options for meth, especially for a pregnant patient, are almost nil. Poland, who is the clinic’s addiction medicine specialist, could rely only on gentle persuasion wrapped around an unflinching truth: that meth use during pregnancy increases the risk of having a smaller baby and of the placenta separating from the uterus, threatening the life of both mother and fetus.
Back then, Sami was living in a shelter, hungry for meth. She loved being a mom. Having to share custody of her first child with her ex was painful enough, but she knew she was in no shape to care for this second baby. Grieving, she placed the infant girl for adoption.
“It still eats at me,” she said.
Like many patients who use multiple substances, Sami has mental disabilities, including attention deficit disorder and bipolar disorder. According to federal data, more than 1 in 4 adults with serious mental disorders turns to illicit drugs. ADHD that has been poorly managed or undiagnosed is particularly common in meth patients.
“It’s almost more notable if they don’t have a disorder,” Poland said. “But sometimes the substance use itself results in mental illness — we call those ‘substance-induced depression’ or ‘substance-induced anxiety.’”


Other risk factors include a history of trauma, a genetic predisposition to addiction or a childhood among relatives dependent on alcohol or drugs. At 3, Sami, who grew up in a one-stoplight town, was in a car accident that left her mother permanently institutionalized with a brain injury. Her father drank heavily, she says; Sami’s descent into addiction began in adolescence with alcohol.
Three years ago, feeling overcome with guilt and shame after placing her daughter for adoption, she slid back into numbing her pain with heroin. And whenever her bipolar disorder medications weren’t balanced and she was feeling depressed, she reached for meth.
By last April, she had enough. “I was in a really, really nasty relationship and my mental health was bad,” she said. “I was so stuck in addiction. I needed help.” During screening for detox and rehab, she discovered she was again pregnant.
She now lives in an apartment that a Grand Rapids nonprofit helped her find, and works as a hotel receptionist. She wants to take this baby home so badly. That goal has helped her avoid meth.
“I won’t even talk to anybody that’s been using,” she said. “I’ve been really diligent, even if that means being lonely sometimes.”
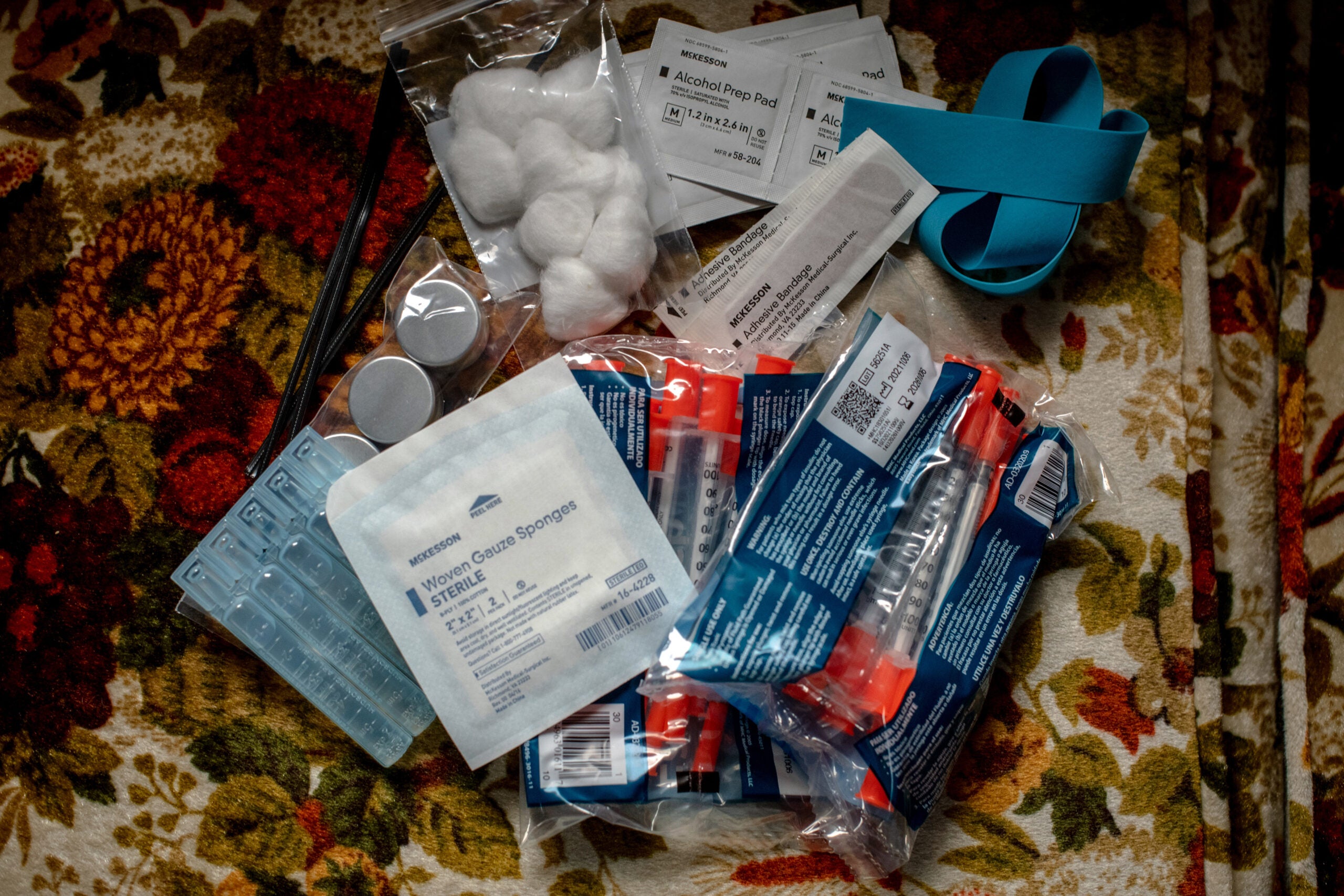
Offering sterile syringes and clean pipes

Twice a week, workers from Kalamazoo Harm Reduction lug a red wagon along rutted trails to the wooded encampments. Pausing to pick up discarded syringes along the paths, they travel from tent to tent, offering free, sterile drug equipment.
They are part of the growing “harm reduction” movement that aims to save lives by preventing overdoses and serious infections.
But the prevalence of so many different drugs has complicated their efforts. The wagon typically holds:
- Packages of 10 short needles, for people still able to hit a fresh vein. Packs of 10 long ones, for those who have to dig around. (Better to use new needles than share used ones.)
- Sterile water for diluting injectable drugs. (Safer than water from the river or a public toilet.)
- Bubbles, the glass stem pipes with bowls for smoking meth. (Better to smoke from your own pipe than take hits from the pipe of someone with cracked, bleeding lips.)


The Street Medicine doctors and harm reduction workers regularly encounter people who swear their meth use is under control but could maybe use help dialing back the fentanyl. And unapologetic meth users, who insist their supply couldn’t possibly contain fentanyl.
“Finding that moment when someone says they’re ready for treatment is hard in all addiction, but meth is making this so much harder,” said Luca, a harm reduction worker who asked to be identified by only a first name because clients are often evading law enforcement. “We had a client who kept missing us on our Monday visits and he finally said, ‘I haven’t known what day it was in so long.’”
So Luca suggested: Maybe after being awake on a four-day meth binge, try a 30-minute nap? “Or we can get you a watch? So while you’re out living your life, you can look down and sort of keep track of where the rest of the world is — and when to meet up with us?”
It is so hard to beat back a beast that is always growing new tentacles. In Western Michigan, as the nights lengthen and temperatures drop, it is becoming harder still, both for people living outdoors, addicted to so many drugs, and those who minister to them.
Soon, the red wagon won’t be able to budge on snow-covered trails. On those days, the Kalamazoo Harm Reduction workers will instead load their safe supplies onto sleds, and set out for the woods.
This article originally appeared in The New York Times.
Extra News Alerts
Get breaking updates as they happen.
Originally posted 2023-11-14 15:37:27.